
Cholesterol Guidelines Finally Got an Update. Here’s What Patients Should Know.
For years, cholesterol conversations have sounded something like this:

And then everyone nods, the visit ends, and the patient goes home wondering:
Okay…but what does that actually mean for me?
That question matters because cholesterol is not just a lab number. It is one of the major risk factors for atherosclerotic cardiovascular disease, or ASCVD.
That is the medical term for plaque buildup in the arteries that can lead to heart attacks, strokes, blocked leg arteries, and other serious vascular problems.
And now, after several years, the major cholesterol guidelines have finally been updated.
The 2026 ACC/AHA Multisociety Dyslipidemia Guideline replaces the 2018 cholesterol guideline and expands the focus beyond “blood cholesterol” to a broader category called dyslipidemia — which includes LDL cholesterol, triglycerides, non-HDL cholesterol, apoB, and lipoprotein(a), also known as Lp(a). The guideline specifically says it retires and replaces the 2018 guideline and was retitled to reflect a broader understanding of cardiovascular risk from lipoproteins beyond LDL alone.
Before we go any further, an important caveat:
I am not a cardiologist. This article is not medical advice, and it is not intended to diagnose, treat, or recommend care for any individual person. My goal here is to review the updated guidelines in plain English so patients can have better, more informed conversations with their own healthcare providers. Decisions about testing, medications, statins, imaging, or treatment goals should always be made with your clinician.
Now let’s break this down.
First, what is dyslipidemia?
Dyslipidemia basically means the fats and fat-carrying particles in your blood are not where we want them to be.
Most people know about LDL cholesterol, often called “bad cholesterol.”
Here is the simple version:
Think of your bloodstream like a highway.
LDL is the delivery truck. It carries cholesterol from the liver out into the body. That is not automatically bad — your body needs cholesterol to build cells and make hormones. But when there is too much LDL traveling around for too long, it can drop cholesterol off where we do not want it: inside the walls of arteries. Over time, that can contribute to plaque buildup.
HDL is often called “good cholesterol.” Think of HDL more like the cleanup crew. It helps carry cholesterol away from the bloodstream and artery walls and back toward the liver, where the body can process it.
So when people say “bad” and “good,” they are oversimplifying — but the basic idea is this:
Too much LDL can contribute to plaque buildup. Higher HDL has traditionally been associated with lower risk, although HDL is not as simple as “the higher, the better.”
And now we know LDL and HDL are not the whole story. The newer guidelines look more broadly at other artery-risk particles too, including triglyceride-rich particles, apoB, non-HDL cholesterol, and lipoprotein(a).
The problem is not just that cholesterol exists. We need cholesterol to survive. The problem is when too many artery-irritating particles are circulating for too long. Over time, those particles can contribute to plaque buildup in the arteries. That plaque can narrow arteries, rupture, or trigger clots — which is how heart attacks and strokes happen.
One of the biggest messages in the new guideline is this:
The longer your arteries are exposed to high-risk cholesterol particles, the more opportunity there is for damage.
That is why the guideline puts more emphasis on earlier screening and earlier intervention.
Put simply:
The longer your arteries are exposed to high-risk cholesterol particles, the more time plaque has to build up. The new guideline is basically saying: let’s not wait until the damage is obvious before we start paying attention.
Why did the guidelines need an update?
The last major guideline was published in 2018.
That may not sound like that long ago, but in medicine, eight years can be a long time. Since then, several things have changed.
We have newer cholesterol-lowering medications. We have more data on non-statin therapies. We have more interest in lipoprotein(a). We have better ways to estimate cardiovascular risk. And we have a growing understanding that “normal enough” cholesterol in middle age may not be the same as “optimal” cholesterol over a lifetime.
In other words:
It was time to catch up.
Big change #1: The new PREVENT risk calculator
The 2018 guideline used what was called the Pooled Cohort Equations to estimate a person’s 10-year risk of cardiovascular disease.
The 2026 guideline now recommends using the newer PREVENT-ASCVD equations for adults ages 30 to 79 who do not already have ASCVD and who have LDL-C levels between 70 and 189 mg/dL. The guideline categorizes risk as low, borderline, intermediate, or high based on this newer tool.
That sounds technical, so here is the plain-English version:
Instead of guessing risk based only on older tools, doctors now have a newer calculator designed to better estimate modern cardiovascular risk.
The guideline describes a “CPR” model:
Calculate the risk.
Personalize the risk using details the calculator may not fully capture.
Reclassify risk when needed, sometimes with coronary artery calcium testing.
This matters because two people can have the same LDL number but very different overall risk. A 35-year-old with a strong family history, elevated Lp(a), and LDL of 165 is not the same as a 35-year-old with LDL of 165 and no other major risk factors.
The number matters. But the person matters too.
Big change #2: LDL goals are back
This is one of the biggest shifts.
The 2018 guideline moved away from strict LDL treatment targets and focused more on statin intensity and percentage reduction.
The 2026 guideline brings back LDL-C and non-HDL-C treatment goals.
The guideline’s own top take-home messages state that LDL-C and non-HDL-C treatment goals are “back” to guide lipid-lowering therapy, while percentage reduction in LDL-C still remains important.
In plain English:
We are not just asking, “Did the LDL go down?”
We are also asking:
Did it go down far enough for this person’s risk level?
For lower-risk people, the goal may be less aggressive. For higher-risk people, the goal may be lower. For people who already have cardiovascular disease, the goal may be lower still.
This is a major patient-facing point because many patients are told, “Your cholesterol is better,” but not necessarily told whether it is at goal for their personal risk category.
Better is good. But sometimes better is not enough.
Big change #3: Lipoprotein(a) testing is now recommended at least once
This is the part many patients have never heard of.
Lipoprotein(a), or Lp(a), is a genetically influenced cholesterol-related particle.
You can eat well, exercise, and do many things right and still have a high Lp(a), because it is largely inherited.
The 2026 guideline recommends that all adults have Lp(a) measured at least once for cardiovascular risk assessment. That is a big deal.
Lp(a) is not part of a standard cholesterol panel in many clinics. You usually have to specifically order it. The guideline notes that Lp(a) levels are mostly genetically determined, usually stay fairly stable over time, and fasting is not required for testing.
So why test it?
Because elevated Lp(a) can identify people whose cardiovascular risk may be higher than their basic cholesterol panel suggests. The guideline says Lp(a) of 125 nmol/L or 50 mg/dL is considered a risk-enhancing factor and is associated with about a 1.4-fold increased cardiovascular risk. Levels around 250 nmol/L or 100 mg/dL are associated with about a 2-fold higher estimated risk.
That does not mean everyone with high Lp(a) is doomed. It means they may need a more serious conversation about controlling the risk factors we can control — especially LDL cholesterol, blood pressure, diabetes, smoking, weight, physical activity, and overall cardiovascular prevention.
In simple language:
Lp(a) is like finding out you inherited a family tendency for plaque buildup. You may not be able to change that inheritance, but you can be much more intentional about controlling the risk factors you can change.
Big change #4: Coronary calcium scoring gets a bigger role
Sometimes the decision to start cholesterol medication is clear. Other times, it is not. That is where coronary artery calcium scoring, or CAC scoring, can help.
A CAC scan is a special CT scan that looks for calcium in the coronary arteries. Calcium can be a marker of plaque buildup.
The 2026 guideline gives CAC scoring a stronger role when treatment decisions are uncertain in intermediate-risk adults and selected borderline-risk adults. The guideline says CAC should be used to further refine risk and guide whether to withhold, postpone, or start lipid-lowering therapy when the decision remains uncertain.
This is not a screening test everyone automatically needs. But it can be useful when the patient and clinician are stuck in the gray zone. For example:
“I am not sure I want to start a statin.”
“My risk calculator number is borderline.”
“My family history worries me.”
“My labs are not terrible, but not great.”
In those situations, CAC can sometimes help answer:
Is there already evidence of plaque in the arteries?
If the answer is yes, the conversation changes.
Big change #5: Earlier screening and earlier intervention
The updated guideline recommends lipid screening starting earlier and continuing regularly.
For adults, screening with a lipid profile is recommended beginning at age 19 and at least every 5 years after that, with more frequent testing for people with additional risk factors.
For children, the guideline recommends lipid screening between ages 9 and 11 if they have not previously been tested, especially to identify familial hypercholesterolemia and other significant lipid disorders.
Why screen kids? Because some cholesterol disorders are inherited.
Familial hypercholesterolemia, often called FH, can cause very high LDL cholesterol from a young age. If it is missed, a person may be exposed to high LDL for decades before anyone realizes there is a problem. The point is not to scare families. The point is to identify people early enough that prevention has a chance to work.
Big change #6: Supplements get called out
This is one patients really need to hear.
The guideline does not recommend dietary supplements to lower LDL-C or triglycerides in people with dyslipidemia because the data are limited, inconsistent, and do not show meaningful cardiovascular risk reduction. This includes many products marketed for “heart health.” That does not mean nutrition does not matter. Nutrition matters tremendously. But supplements are not the same as evidence-based treatment. There is a difference between:
“I am eating more fiber-rich foods, vegetables, nuts, legumes, and whole grains.”
and
“I bought a bottle of something from the supplement aisle that claims to clean my arteries.”
Those are not the same thing.
Big change #7: More medication options exist now
Statins remain the foundation of cholesterol-lowering therapy for many patients. But they are no longer the only tools in the toolbox. The 2026 guideline spends more time discussing non-statin medications.
Statins are still the main starting point for many patients because they have the strongest track record for lowering LDL cholesterol and reducing heart attack and stroke risk. But some patients need additional medications to reach their cholesterol goals. Others may not tolerate statins well and may need a different approach.
Here is the “for dummies” version:
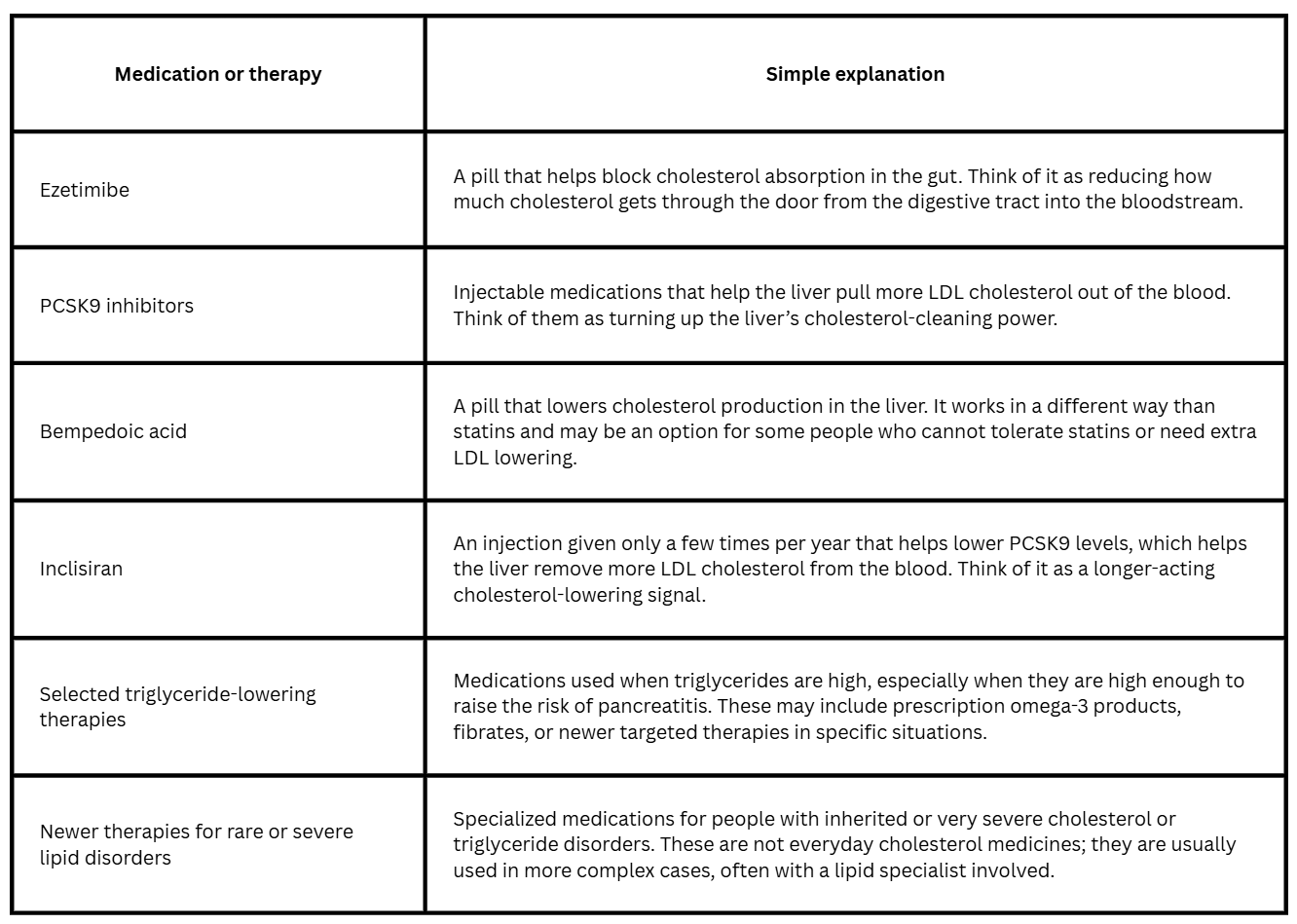
The big point is this:
Statins are still the foundation for many patients, but they are not the only option. The updated guideline recognizes that cholesterol care is becoming more personalized — based on a person’s risk, goals, side effects, genetics, cost, access, and what they can realistically tolerate.
What changed from 2018 to 2026?
Here is the practical compare-and-contrast version:
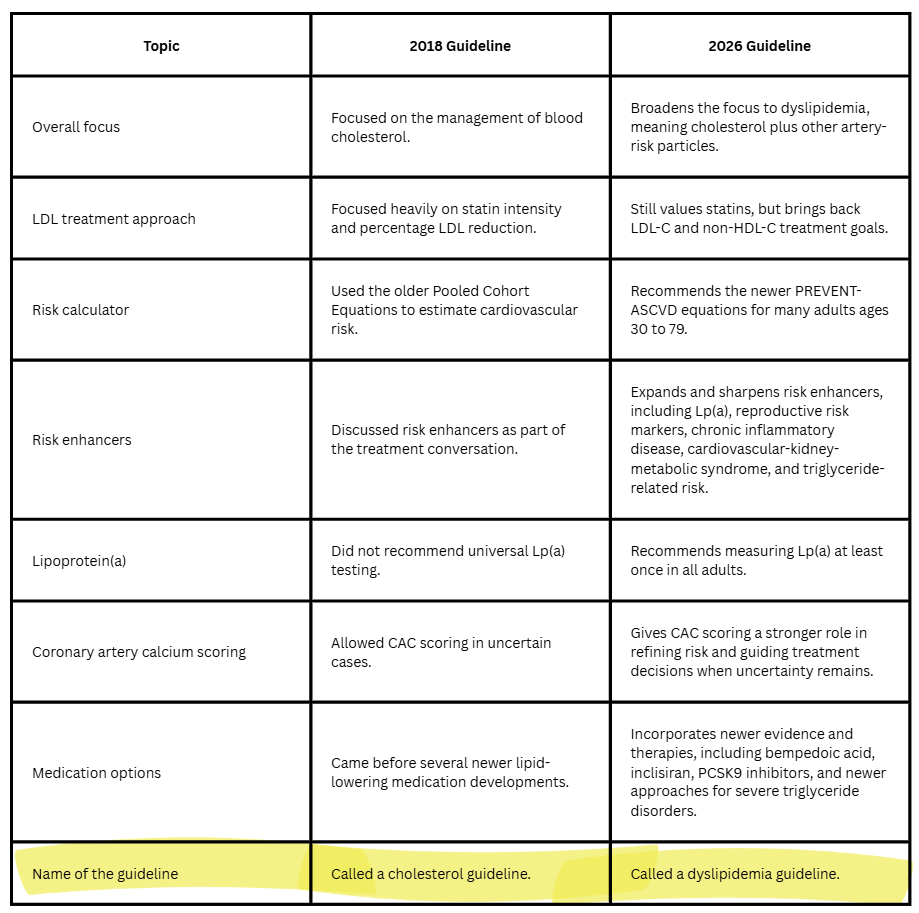
That last line - the name change - matters. It tells us the field is no longer thinking only about “cholesterol.” It is thinking about the broader set of particles that contribute to cardiovascular risk.
What patients should ask at their next visit
This is where patients can turn a confusing guideline into a practical conversation. You do not need to walk into your doctor’s office quoting guideline tables. But you can ask better questions. Try these:
What is my LDL cholesterol?
What is my non-HDL cholesterol?
Based on my personal risk, do I have a goal number?
Should my risk be calculated using the PREVENT-ASCVD calculator?
Should I have lipoprotein(a) checked once?
Do I have any risk factors that change the conversation?
Would a coronary calcium score help clarify my risk, or is my treatment decision already clear?
If I am not at goal, what are my options besides “try harder”?
That last question is important.
Patients are often told to “work on lifestyle,” and lifestyle absolutely matters. But when cholesterol is driven by genetics, age, diabetes, kidney disease, inflammatory disease, or inherited lipid disorders, lifestyle may not be enough by itself. That is not failure. That is biology.
The bottom line
The new cholesterol guidelines are not really just about cholesterol. They are about risk, and they are about time. They are about identifying people earlier, understanding their individual risk more clearly, and treating aggressively enough when the risk is high. For patients, the big takeaway is this:
Do not settle for being told your cholesterol is “fine” or “a little high” without understanding what that means for you.
Your LDL number matters. Your non-HDL cholesterol matters. Your family history matters. Your diabetes, kidney disease, inflammatory conditions, pregnancy history, smoking history, blood pressure, and Lp(a) may matter.
And if there is uncertainty, tools like the PREVENT-ASCVD calculator and coronary calcium scoring may help guide the conversation.
The goal is not to turn every patient into a cardiologist. The goal is to help patients ask better questions. Because when patients understand the “why” behind the lab numbers, they are much better prepared to participate in decisions about their own care.